Practically relevant classification that helps in management
- Grade 1a – Puffy nipple
- Grade 1b – small amount of fat limited to lower half + puffy nipple . fat less than 250 ml
- Grade 2a – fat over entire breast, no axillary fat or breast rolls
- Grade 2b – fat over entire breast, no axillary fat or breast rolls , loose skin , saggy skin with the need for skin lift ( < 500 ml fat)
- Grade 3a – large amount of fat with visible female breast look, with or without breast rolls ( > 500 ml to 1000 ml)
- Grade 3b – large amount of fat with visible female type breast and breast rolls
- Grade 4a – very large breast, not in shape with the body at all, looseness of skin. Breast rolls present ( more than 1000 ml fat)
- Grade 4b – very large breast, not in shape with chest at all , with skin looseness due to weight loss. The problem is loose saggy skin and not much fat . Breast rolls present
Divine Clinical Classification Of Gynecomastia
| Grade | Procedure | Description | Infiltration | Treatment plan |
| 1a | Puffy Nipple | No obvious problem is visible except stretched areola. Button type feel below | 50 ml each side along with the gland | Excision in LA from the infraareolar incision |
| 1b | Minor chest enlargement (< 100 ml fat, gland +) | The chest is a visibly bigger, but limited fat, usually higher amount of fibro-glandular tissue | 200 ml each side | Suction and gland excision in LA from infraareolar incision and stab incision in the inframammary area |
| 1c | Minor chest enlargement (100-250 gm fat) | The chest is visibly larger. Assessed fat component is between 100 to 250 gm | 300 ml each side | Suction and gland excision In GA from infraareolar incision and stab incision in the axillary area |
| 2a | Moderate chest enlargement | The chest is moderately enlarged. The fat component is between 250-500 gm. No skin looseness expected | 500 ml each side | Suction – stab incision in axillary area, and gland excision In GA from the infraareolar incision |
| 2b | Moderate chest enlargement with skin looseness | The chest is moderately enlarged. The fat component is between 250-500 gm.. large gland component in the form of a conical chest. Excision is likely to leave loose skin. U lift needed | 500 ml each side | Suction from stab incision in axillary area, and gland excision + U skin lift from supra areolar approach In GA |
| 3a | Big chest with side rolls without skin looseness | The chest is severely enlarged. The fat component is between 500+ gm. Fat in breast rolls+. No skin looseness expected | 750 ml each side and axilla | Suction – stab incision in axillary area, axilla from infra areolar, and gland excision In GA from the infraareolar incision |
| 3b | Big chest with side rolls with skin looseness expected | The chest is severely enlarged, fat component +, axilla rolls +, skin looseness expected | 750 ml each side and axilla | Suction from stab incision in axillary area, and gland excision + U skin lift from supra areolar approach In GA |
| 4a | Big chest with very large skin laxity | The chest is severely enlarged, fat component +, axilla rolls + large skin looseness expected | 750 ml + each side | Stage procedure. 1st stage sams as 3b. 2nd stage, o- lift procedure |
| 4b | Severe weight loss condition | The chest is hanging, not much fat excess expected, gland +, skin excess ++ | 200-250 each side | Mastopexy, chest lift type of procedure |
Why is it necessary to have a new classification for gynecomastia?
The previous classifications have taken a very simplistic view of gynecomastia, this condition occurs in myriad forms and have specific treatment planning for each grade.
- This classification clearly defines what is possible in local anesthesia and what is recommended under general anesthesia.
- It talks of managing potential complications and gives a separate grade to it
- Asymmetric gynecomastia has not been discussed previously since the treatment can be remarkably different for both the sides
- Unilateral gynecomastia has not been discussed previously
- Severe skin laxity has not been discussed in any classification
- Post weight loss gynecomastia correction has been included
- Puffiness of nipple has not been identified as a separate grade. It is important since the treatment is absolutely different compared to all other grades
- Only projecting nipple and areola
- No fat
- No breast rolls
- No axillary breast
- No skin laxity
- Is sometimes painful
- Amenable to be performed under local anesthesia
- Fat is limited to just under the areola and lower quadrant of the breast – check by Pectoralis muscle contraction
- Gland is usually present
- No skin laxity
- No breast rolls
- Less than 250 ml fat
- No axillary breast
- Amenable to be performed under local anesthesia with liposuction and gland removal
- Fat over entire breast – check with Pectoralis muscle contraction
- Gland usually present
- 250 – 500 ml fat
- No skin laxity
- No breast rolls
- No axillary breast
- Patient will probably need to be operated in general anesthesia
- Only projecting nipple and areola
- No fat
- No breast rolls
- No axillary breast
- No skin laxity
- Is sometimes painful
- Amenable to be performed under local anesthesia
- Excess fat ( mroe than 500 ml fat , less than 1000 ml fat)
- Typical female small breast look
- Gland usually present
- No skin laxity
- No breast rolls
- No axillary breast
- Patient with need GA
- As in grade 3a , with breast rolls , and skin laxity needing a u lift
- Breast rolls +
- Axillary breast may or may not, but usually is
- No significant skin laxity
- Large amount of fat ( > 1000 ml )
- Gland usually present
- As in grade 4a, with skin laxity needing a skin lift procedure
Advantages of this new classification
- No need for ultrasound examination
- Teachable
- Standard Treatment Protocols
- Predictable Results
- Several clinical situations not discussed previously included
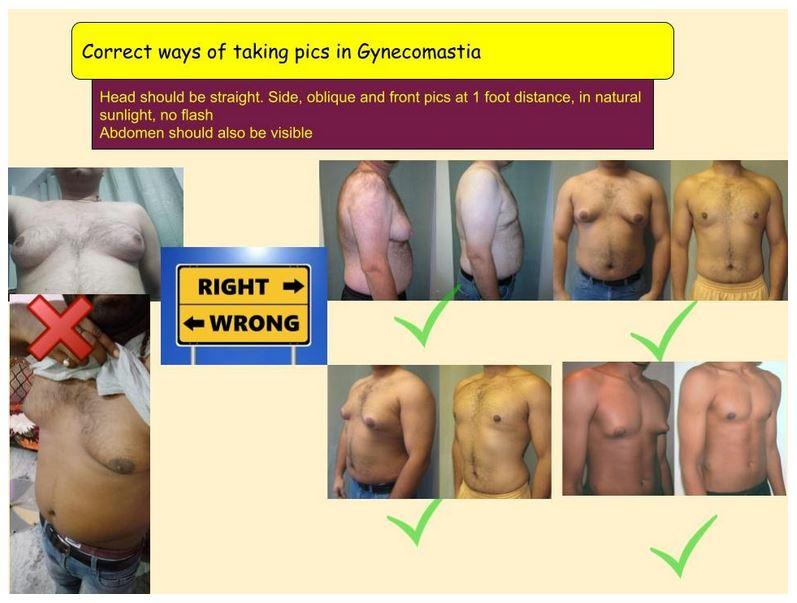
Photography in Gynecomastia

The pictures need to be
- From front – 3 feet away from the patient – assess the grade
- From side – exactly 90 degrees – both sides – assess sde roles
- Angle – 45 degrees from both sides